Mesothelioma Histology: 2025 Guide to Diagnosis & Types
Mesothelioma, a rare and aggressive cancer primarily affecting the lining of the lungs, abdomen, or heart, presents a significant diagnostic challenge. Accurate diagnosis is paramount for effective treatment planning and predicting patient outcomes. Histology, the microscopic examination of tissue samples, plays a crucial role in confirming mesothelioma and distinguishing it from other, more common conditions. This 2025 guide provides an in-depth look at mesothelioma histology, focusing on the diagnostic process, different histological subtypes, and the latest advancements in this field.
The complexity of mesothelioma diagnosis stems from its variable presentation and the potential for mimicking other diseases. Histological examination is often combined with immunohistochemistry (IHC), a technique that uses antibodies to identify specific proteins in tissue samples, further refining the diagnosis. This guide will delve into the specific IHC markers used in mesothelioma diagnosis and their significance in differentiating mesothelioma from its mimics, such as adenocarcinoma and reactive mesothelial proliferations.
This article aims to serve as a comprehensive resource for pathologists, oncologists, and other healthcare professionals involved in the diagnosis and management of mesothelioma. By understanding the nuances of mesothelioma histology, clinicians can improve diagnostic accuracy, guide treatment decisions, and ultimately enhance patient care. We will explore the key histological features of each mesothelioma subtype, discuss the diagnostic challenges encountered in practice, and highlight the evolving role of molecular diagnostics in the future of mesothelioma diagnosis.
Understanding Mesothelioma Histology: A Foundation
Histology is the cornerstone of mesothelioma diagnosis. It involves obtaining a tissue sample, typically through biopsy or surgery, and processing it for microscopic examination. The pathologist then analyzes the cellular architecture, nuclear features, and other morphological characteristics of the tissue to determine if it is consistent with mesothelioma. The process includes:
- Tissue Acquisition: Obtaining a representative tissue sample is crucial. This can be achieved through various methods, including needle biopsy, thoracoscopy (for pleural mesothelioma), laparoscopy (for peritoneal mesothelioma), or open surgical biopsy.
- Tissue Processing: The tissue sample is fixed (usually in formalin), embedded in paraffin wax, and then thinly sliced into sections.
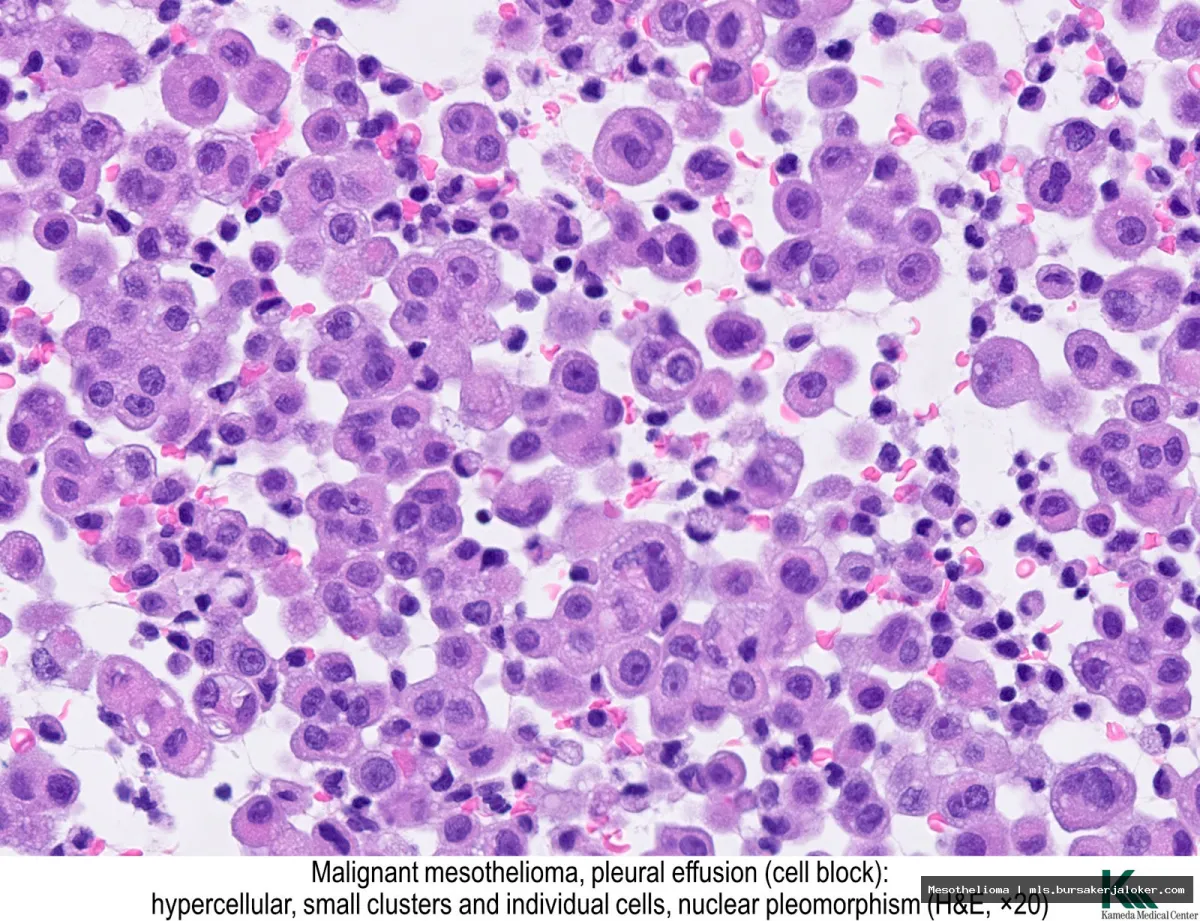
- Staining: The tissue sections are stained with dyes, such as hematoxylin and eosin (H&E), to highlight cellular structures and allow for microscopic visualization.
- Microscopic Examination: The pathologist examines the stained tissue sections under a microscope to identify characteristic features of mesothelioma.
Key Histological Features to Look For
When examining a tissue sample for mesothelioma, pathologists look for specific features that are indicative of the disease. These include:
- Growth Pattern: Mesothelioma can exhibit various growth patterns, including epithelioid, sarcomatoid, and biphasic (a combination of both).
- Cellular Morphology: The shape and appearance of the cells themselves are important. Epithelioid mesothelioma cells are typically polygonal or cuboidal with abundant cytoplasm, while sarcomatoid cells are spindle-shaped and resemble fibroblasts.
- Nuclear Features: The size, shape, and staining properties of the cell nuclei are also examined. Mesothelioma cells often have large, irregular nuclei with prominent nucleoli.
- Invasion: Mesothelioma tends to invade surrounding tissues and structures.
Mesothelioma Subtypes: A Histological Perspective
Mesothelioma is classified into several subtypes based on its histological appearance. The most common subtypes are epithelioid, sarcomatoid, and biphasic. Understanding these subtypes is essential for accurate diagnosis and prognosis.
Epithelioid Mesothelioma
Epithelioid mesothelioma is the most common subtype, accounting for approximately 50-70% of all cases. Its key histological features include:
- Cell Shape: Polygonal or cuboidal cells with abundant cytoplasm.
- Growth Pattern: Can exhibit various growth patterns, including tubular, papillary, and solid.
- Nuclear Features: Large, irregular nuclei with prominent nucleoli.
- Cytoplasmic Features: May contain vacuoles or eosinophilic inclusions.
Several variants of epithelioid mesothelioma exist, including:
- Tubulopapillary: Characterized by tubules and papillary structures lined by epithelioid cells.
- Adenomatoid: Mimics adenocarcinoma due to its glandular appearance.
- Clear Cell: Contains cells with clear cytoplasm.
- Deciduoid: Resembles decidual cells of the pregnant uterus.
Sarcomatoid Mesothelioma
Sarcomatoid mesothelioma is a less common subtype, accounting for approximately 10-20% of all cases. It is characterized by:
- Cell Shape: Spindle-shaped cells resembling fibroblasts.
- Growth Pattern: Fascicular or storiform (whorled) pattern.
- Nuclear Features: Elongated nuclei with less prominent nucleoli compared to epithelioid mesothelioma.
- Cytoplasmic Features: Less abundant cytoplasm than epithelioid mesothelioma.
Sarcomatoid mesothelioma can be challenging to diagnose because it can resemble other sarcomas. Immunohistochemistry is particularly important in differentiating sarcomatoid mesothelioma from other spindle cell tumors.
Biphasic Mesothelioma
Biphasic mesothelioma contains both epithelioid and sarcomatoid components. The proportion of each component can vary significantly from case to case. Diagnosis requires careful evaluation of both components and their spatial relationship. The presence of both distinct epithelioid and sarcomatoid areas is crucial for the diagnosis.
Other Rare Mesothelioma Subtypes
In addition to the three main subtypes, several rare variants of mesothelioma exist, including:
- Desmoplastic Mesothelioma: Characterized by dense collagenous stroma and scattered atypical cells.
- Small Cell Mesothelioma: Composed of small, round, or oval cells with scant cytoplasm.
- Lymphohistiocytoid Mesothelioma: Exhibits a prominent inflammatory infiltrate composed of lymphocytes and histiocytes.
Immunohistochemistry (IHC) in Mesothelioma Diagnosis
Immunohistochemistry (IHC) is an essential tool in mesothelioma diagnosis, particularly in challenging cases. IHC involves using antibodies to detect specific proteins in tissue samples, allowing pathologists to differentiate mesothelioma from other tumors, such as adenocarcinoma and reactive mesothelial proliferations.
Positive IHC Markers for Mesothelioma
Several IHC markers are typically positive in mesothelioma, including:
- Calretinin: A calcium-binding protein highly expressed in mesothelioma.
- WT1: A transcription factor involved in cell growth and differentiation.
- D2-40 (Podoplanin): A transmembrane glycoprotein.
- CK5/6: A high molecular weight cytokeratin.
- Mesothelin: A cell surface glycoprotein.
Negative IHC Markers for Mesothelioma
Certain IHC markers are typically negative or weakly expressed in mesothelioma, helping to distinguish it from adenocarcinoma. These include:
- CEA (Carcinoembryonic Antigen): Strongly expressed in adenocarcinoma.
- TTF-1 (Thyroid Transcription Factor-1): Expressed in lung adenocarcinoma.
- Napsin A: Expressed in lung adenocarcinoma.
IHC Panels for Mesothelioma Diagnosis
Pathologists often use IHC panels, which are combinations of several antibodies, to improve diagnostic accuracy. A typical IHC panel for mesothelioma diagnosis may include:
- Calretinin, WT1, D2-40, CK5/6 (positive markers)
- CEA, TTF-1, Napsin A (negative markers)
The specific IHC panel used may vary depending on the clinical context and the pathologist’s preference. For more information, you can refer to Mesothelioma as an additional resource.
Diagnostic Challenges and Pitfalls
Despite advancements in diagnostic techniques, mesothelioma diagnosis can still be challenging. Several factors can contribute to diagnostic difficulties, including:
Sampling Issues
The quality and representativeness of the tissue sample are crucial for accurate diagnosis. Small or poorly preserved samples may not contain sufficient diagnostic material. Furthermore, biopsies may not accurately reflect the overall tumor heterogeneity, leading to misdiagnosis.
Differential Diagnoses
Mesothelioma can mimic other diseases, such as adenocarcinoma, reactive mesothelial proliferations, and other sarcomas. Distinguishing mesothelioma from these conditions requires careful evaluation of histological features and IHC results.
Interobserver Variability
Pathological interpretation can be subjective, and interobserver variability (differences in interpretation between pathologists) can occur. Second opinions from experienced pathologists specializing in mesothelioma can be valuable in challenging cases.
The Future of Mesothelioma Histology: Molecular Diagnostics
Molecular diagnostics are playing an increasingly important role in mesothelioma diagnosis and management. Molecular techniques, such as next-generation sequencing (NGS), can identify genetic alterations that are specific to mesothelioma and may have prognostic or therapeutic implications.
BAP1 Mutations
Mutations in the BAP1 gene are common in mesothelioma and are associated with improved prognosis. BAP1 immunohistochemistry can be used to detect loss of BAP1 protein expression, which is indicative of BAP1 mutation.
NF2 Mutations
Mutations in the NF2 gene are also frequently observed in mesothelioma and may be associated with specific histological subtypes.
Molecular Subtyping
Molecular profiling can be used to classify mesothelioma into distinct molecular subtypes, which may have different clinical behaviors and responses to therapy. These advancements are helping to personalize treatment strategies for mesothelioma patients.
Conclusion
Mesothelioma histology remains a critical component of the diagnostic process. By understanding the histological subtypes, utilizing immunohistochemistry, and staying abreast of the latest advancements in molecular diagnostics, pathologists and oncologists can improve diagnostic accuracy, guide treatment decisions, and ultimately improve outcomes for patients with this challenging disease. This 2025 guide provides a comprehensive overview of the current state of mesothelioma histology, offering valuable insights for healthcare professionals involved in the diagnosis and management of this rare cancer.
Conclusion
In summary, mesothelioma histology plays a critical role in the diagnosis and management of this aggressive cancer. Accurate identification of the specific histological subtype – epithelioid, sarcomatoid, or biphasic – is paramount for determining prognosis and tailoring treatment strategies. Through careful microscopic examination and the application of immunohistochemical stains, pathologists can differentiate mesothelioma from other malignancies and provide clinicians with the essential information needed for informed decision-making. The challenges inherent in diagnosing mesothelioma, particularly in distinguishing it from benign reactive mesothelial proliferations and other cancers, underscore the importance of expert pathological review and adherence to established diagnostic criteria.
Ultimately, a comprehensive understanding of mesothelioma histology is vital for both pathologists and clinicians involved in the care of patients with this disease. Continued research aimed at identifying novel diagnostic markers and refining histological classification is crucial for improving patient outcomes. We encourage healthcare professionals to stay abreast of the latest advancements in mesothelioma diagnosis and treatment and to consult with experienced pathologists when encountering challenging cases. For further information on mesothelioma and its histological subtypes, please visit the National Cancer Institute website at https://www.cancer.gov.
Frequently Asked Questions (FAQ) about mesothelioma histology
What are the three main histological subtypes of mesothelioma, and how do they differ under a microscope?
The three primary histological subtypes of mesothelioma are epithelioid, sarcomatoid, and biphasic. The epithelioid subtype is the most common and is characterized by cells that resemble epithelial cells, often arranged in tubular, papillary, or solid patterns. Under a microscope, these cells typically have distinct cell borders, abundant cytoplasm, and round to oval nuclei. The sarcomatoid subtype is less common and consists of spindle-shaped cells that resemble fibroblasts, often arranged in fascicles or sheets. These cells usually have elongated nuclei and less cytoplasm compared to epithelioid cells. Finally, the biphasic subtype contains a mixture of both epithelioid and sarcomatoid features within the same tumor. Accurate identification of these subtypes is crucial for prognosis and treatment planning, and requires careful microscopic evaluation by a pathologist.
How is immunohistochemistry used in diagnosing mesothelioma, and what are some common markers used to differentiate it from other cancers?
Immunohistochemistry (IHC) plays a vital role in the diagnosis of mesothelioma, especially in differentiating it from other cancers that can mimic its appearance, such as adenocarcinoma and squamous cell carcinoma. IHC involves using antibodies to detect specific proteins within tissue samples. Several markers are commonly used. Calretinin, WT1, D2-40, and CK5/6 are typically positive in mesothelioma, while markers like CEA, MOC-31, Ber-EP4, and TTF-1 are usually positive in adenocarcinoma. The specific panel of antibodies used will depend on the clinical scenario and the initial histological findings. A panel of both positive and negative markers is typically required for accurate diagnosis. The pathologist will carefully analyze the staining patterns to arrive at a definitive diagnosis. Using IHC helps to provide a more specific and accurate diagnosis of mesothelioma.
What are some histological features that suggest a poor prognosis in mesothelioma, and how do these features influence treatment decisions?
Certain histological features of mesothelioma are associated with a poorer prognosis. The sarcomatoid subtype generally carries a worse prognosis than the epithelioid subtype. High mitotic activity (a measure of cell division) and necrosis (tissue death) within the tumor are also indicators of more aggressive disease. Furthermore, the presence of certain growth patterns, such as a solid growth pattern in epithelioid mesothelioma, can suggest a less favorable outcome. These histological findings influence treatment decisions by helping oncologists determine the aggressiveness of the disease and the likelihood of response to different therapies. For example, sarcomatoid mesothelioma may be less responsive to certain chemotherapies compared to epithelioid mesothelioma, potentially leading to the consideration of alternative treatment options, such as clinical trials or more aggressive surgical approaches. Ultimately, histological findings are considered alongside other clinical and imaging data to formulate the most appropriate treatment plan.