Mesothelioma Pathology Outlines 2025: A Complete Guide
Navigating the complexities of mesothelioma diagnosis can be daunting, even for seasoned pathologists. Accurate identification and classification are crucial for effective treatment planning and predicting patient outcomes. The “Mesothelioma Pathology Outlines” serve as invaluable resources, providing a comprehensive framework for understanding the various aspects of this challenging disease. This article, anticipating the landscape of 2025, aims to offer a complete guide to these outlines, highlighting key diagnostic features, evolving classifications, and the growing importance of molecular testing.
The field of mesothelioma pathology is constantly evolving, driven by advancements in research and technology. New diagnostic markers are being discovered, and our understanding of the disease’s molecular underpinnings is deepening. Staying abreast of these changes is essential for pathologists to provide accurate and timely diagnoses. This guide will delve into the core components of the Mesothelioma Pathology Outlines, focusing on the most relevant and up-to-date information for 2025, including the latest WHO classification updates and emerging diagnostic techniques.
This article isn’t just a summary of existing information; it’s a practical roadmap for navigating the complexities of mesothelioma diagnosis. We’ll explore the different subtypes of mesothelioma, the key histological features that distinguish them, and the ancillary techniques that can aid in diagnosis. We will also discuss the challenges and pitfalls of mesothelioma diagnosis, and provide strategies for avoiding common errors. Ultimately, this guide aims to empower pathologists with the knowledge and tools they need to provide the best possible care for patients with mesothelioma.
Understanding Mesothelioma: An Overview
Mesothelioma is a rare and aggressive cancer that arises from the mesothelial cells lining the pleura (lung lining), peritoneum (abdominal lining), or pericardium (heart lining). The most common type is pleural mesothelioma, linked to asbestos exposure. Accurate diagnosis is critical for treatment planning, as different subtypes have varying prognoses and respond differently to therapies.
Etiology and Risk Factors
The primary risk factor for mesothelioma is exposure to asbestos. Asbestos fibers, when inhaled or ingested, can become lodged in the mesothelial tissues, leading to chronic inflammation and eventually malignant transformation. The latency period between asbestos exposure and the development of mesothelioma can be decades, often 20-50 years. Other potential risk factors, though less common, include exposure to erionite (a fibrous mineral) and certain genetic predispositions.
Common Sites of Mesothelioma
While pleural mesothelioma is the most frequently encountered form, it’s important to recognize that mesothelioma can also occur in other locations:
- Pleural Mesothelioma: Affects the lining of the lungs.
- Peritoneal Mesothelioma: Affects the lining of the abdomen.
- Pericardial Mesothelioma: Affects the lining of the heart (very rare).
- Tunica Vaginalis Mesothelioma: Affects the lining of the testicles (extremely rare).
Histological Subtypes of Mesothelioma
The World Health Organization (WHO) classification of mesothelioma recognizes several histological subtypes, each with distinct morphological features and prognostic implications. Accurate subtyping is essential for guiding treatment decisions.
Epithelioid Mesothelioma
Epithelioid mesothelioma is the most common subtype, accounting for approximately 50-70% of cases. It is characterized by neoplastic cells that resemble epithelial cells, forming tubules, papillae, or solid sheets. Key features include:
- Cell Morphology: Cells are typically cuboidal or polygonal with abundant cytoplasm and distinct cell borders.
- Nuclear Features: Nuclei are usually round to oval with prominent nucleoli.
- Growth Patterns: Can exhibit various growth patterns, including tubular, papillary, solid, and trabecular.
- Immunohistochemistry: Typically positive for mesothelial markers (calretinin, WT1, D2-40) and negative for adenocarcinoma markers (CEA, Ber-EP4).
Sarcomatoid Mesothelioma
Sarcomatoid mesothelioma is characterized by spindle-shaped cells that resemble fibroblasts or sarcomas. It is generally associated with a poorer prognosis than epithelioid mesothelioma. Key features include:
- Cell Morphology: Cells are elongated and spindle-shaped with scant cytoplasm.
- Nuclear Features: Nuclei are often hyperchromatic and pleomorphic.
- Growth Patterns: Typically exhibits a fascicular or storiform growth pattern.
- Immunohistochemistry: Can be challenging to diagnose due to variable expression of mesothelial markers. Often requires a panel of antibodies to exclude other sarcomas.
Biphasic Mesothelioma
Biphasic mesothelioma contains both epithelioid and sarcomatoid components. The relative proportion of each component can vary significantly. The prognosis is generally intermediate between epithelioid and sarcomatoid mesothelioma. Key features include:
- Dual Morphology: Presence of both epithelioid and sarcomatoid areas within the same tumor.
- Prognostic Implications: Prognosis is influenced by the proportion of sarcomatoid component; a higher proportion is associated with a worse outcome.
- Diagnostic Challenges: Careful sampling is crucial to ensure both components are represented in the biopsy.
Desmoplastic Mesothelioma
Desmoplastic mesothelioma is a rare variant characterized by dense collagenous stroma with scattered atypical spindle cells. It can be easily mistaken for benign fibrous tissue or other sarcomas. Key features include:
- Prominent Stroma: Abundant collagenous stroma that dominates the microscopic appearance.
- Sparse Cellularity: Few atypical spindle cells scattered within the stroma.
- Diagnostic Difficulty: Requires careful assessment to differentiate from benign conditions and other sarcomas.
- Immunohistochemistry: Mesothelial markers may be focally positive or even negative, adding to the diagnostic challenge.
Other Rare Subtypes
While less common, it’s important to be aware of other rare subtypes of mesothelioma including:
- Small Cell Mesothelioma: Resembles small cell carcinoma.
- Clear Cell Mesothelioma: Characterized by clear cytoplasm.
- Deciduoid Mesothelioma: Mimics decidual cells.
Diagnostic Techniques in Mesothelioma Pathology
Accurate diagnosis of mesothelioma requires a combination of histological examination, immunohistochemistry, and, increasingly, molecular testing.
Histological Examination
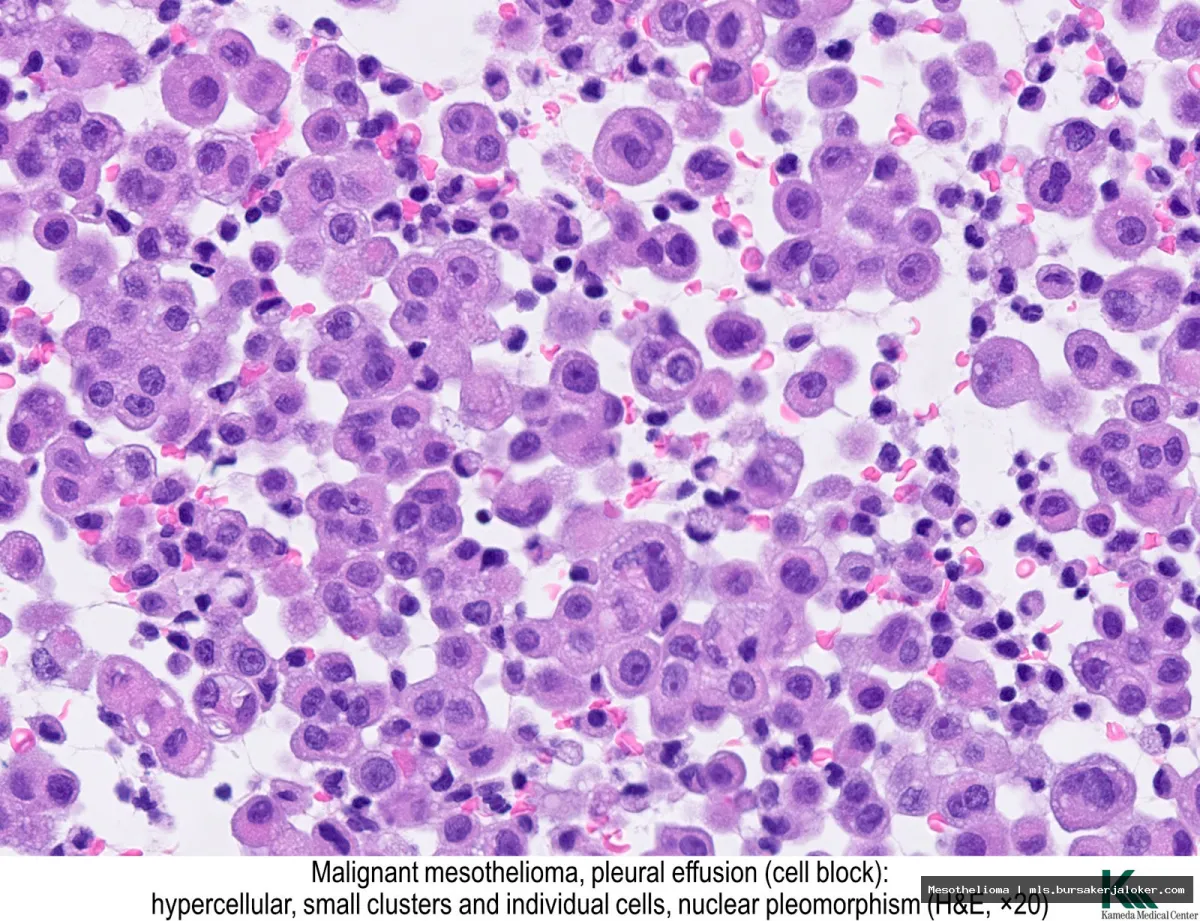
The initial step in diagnosing mesothelioma is careful examination of tissue biopsies or cytology specimens. The pathologist assesses the cellular morphology, growth patterns, and stromal features to determine if the tissue is consistent with mesothelioma and to classify the subtype.
Immunohistochemistry (IHC)
Immunohistochemistry is a crucial ancillary technique used to confirm the mesothelial origin of the tumor and to distinguish it from other malignancies, particularly adenocarcinomas. A panel of antibodies is typically used, including:
- Positive Mesothelial Markers: Calretinin, WT1, D2-40 (podoplanin), CK5/6
- Negative Adenocarcinoma Markers: CEA, Ber-EP4, MOC-31
It’s important to note that no single marker is completely specific for mesothelioma, and a panel approach is necessary for accurate diagnosis. Furthermore, the expression of these markers can vary depending on the subtype of mesothelioma.
Molecular Testing
Molecular testing is playing an increasingly important role in the diagnosis and management of mesothelioma. It can be used to:
- Confirm Diagnosis: Detect specific genetic alterations associated with mesothelioma, such as BAP1 mutations and CDKN2A deletions.
- Predict Prognosis: Identify molecular markers that are associated with different survival outcomes.
- Guide Treatment: Identify patients who may be eligible for targeted therapies.
Fluorescence in situ hybridization (FISH) and next-generation sequencing (NGS) are commonly used molecular techniques in mesothelioma pathology.
Differential Diagnosis of Mesothelioma
Mesothelioma can be challenging to diagnose, as it can mimic other malignancies and benign conditions. The most important differential diagnoses include:
Adenocarcinoma
Distinguishing epithelioid mesothelioma from adenocarcinoma is a common diagnostic challenge. Immunohistochemistry plays a crucial role in differentiating these two entities. Adenocarcinomas are typically positive for CEA, Ber-EP4, and MOC-31, while mesotheliomas are typically positive for calretinin, WT1, and D2-40.
Sarcomas
Sarcomatoid mesothelioma can be difficult to distinguish from other sarcomas, particularly those that arise in the pleura or peritoneum. Immunohistochemistry and molecular testing are essential for accurate diagnosis. A panel of antibodies specific for sarcomas, such as smooth muscle actin (SMA), desmin, and S100, should be used to exclude other sarcoma subtypes.
Reactive Mesothelial Hyperplasia
Reactive mesothelial hyperplasia can mimic mesothelioma, particularly in cytology specimens. Key features that favor reactive hyperplasia include bland nuclear features, absence of mitotic activity, and presence of inflammation. For more information, you can refer to Mesothelioma as an additional resource.
Challenges and Pitfalls in Mesothelioma Diagnosis
Mesothelioma diagnosis presents several challenges, including:
- Limited Tissue Samples: Biopsies are often small and fragmented, making it difficult to assess the overall architecture of the tumor.
- Heterogeneity: Mesothelioma can exhibit significant heterogeneity, with different areas of the tumor showing different morphological features.
- Variable Marker Expression: The expression of mesothelial markers can vary depending on the subtype of mesothelioma and the antibody used.
- Subjectivity: Interpretation of histological features and immunohistochemical results can be subjective, leading to interobserver variability.
The Future of Mesothelioma Pathology: 2025 and Beyond
The field of mesothelioma pathology is poised for significant advancements in the coming years. We can expect to see:
- Improved Diagnostic Markers: The discovery of new and more specific diagnostic markers for mesothelioma.
- Advanced Molecular Testing: Wider adoption of NGS and other advanced molecular techniques for diagnosis, prognosis, and treatment selection.
- Artificial Intelligence (AI): The use of AI to assist pathologists in the diagnosis and classification of mesothelioma.
- Personalized Medicine: The development of personalized treatment strategies based on the molecular characteristics of the tumor.
By staying informed about these advancements and utilizing the resources provided by the Mesothelioma Pathology Outlines, pathologists can play a crucial role in improving the diagnosis and management of this challenging disease.
Conclusion
In summary, mesothelioma pathology outlines serve as an invaluable resource for pathologists in the accurate diagnosis and classification of this challenging malignancy. By providing a structured framework encompassing key diagnostic criteria, immunohistochemical markers, and molecular features, these outlines promote consistency and standardization in reporting. This enhanced clarity is crucial for optimal patient management, influencing treatment strategies and prognostic predictions in a disease with a complex and variable clinical course. Adherence to these guidelines is paramount for ensuring accurate and reproducible diagnoses.
The information presented herein highlights the importance of staying current with the latest advancements in mesothelioma pathology. Given the evolving understanding of this disease, it is essential for pathologists to continually update their knowledge and refine their diagnostic approaches. We encourage all practitioners involved in mesothelioma diagnosis to utilize and contribute to the ongoing development of comprehensive pathology outlines. For further information and access to updated resources, please visit the official websites of organizations dedicated to mesothelioma research and pathology, such as the International Mesothelioma Interest Group and the College of American Pathologists. Learn more at CAP.org.
Frequently Asked Questions (FAQ) about mesothelioma pathology outlines
What information is typically included in a mesothelioma pathology outline, and why is it important for diagnosis and treatment planning?
A mesothelioma pathology outline provides a structured and comprehensive summary of the microscopic and macroscopic features observed in a tissue sample obtained from a suspected mesothelioma case. Key information includes the tumor’s location, size, and growth pattern, as well as the specific histological subtype (e.g., epithelioid, sarcomatoid, biphasic). The outline details cellular characteristics such as nuclear features, mitotic activity, and the presence of necrosis. Immunohistochemical stains, which help differentiate mesothelioma from other cancers, are also documented, including markers like calretinin, WT1, and CK5/6. Accurate diagnosis and subtyping are critical because they directly influence treatment options and prognosis. The pathology outline serves as a vital communication tool between pathologists, oncologists, and other healthcare professionals involved in patient care, ensuring a consistent and informed approach to management.
How do pathologists use immunohistochemistry (IHC) markers in mesothelioma pathology outlines to differentiate mesothelioma from other types of cancer, particularly adenocarcinoma?
Immunohistochemistry (IHC) is crucial for distinguishing mesothelioma from other cancers, especially adenocarcinoma, which can mimic mesothelioma’s appearance under the microscope. Pathologists utilize a panel of IHC markers, documented in the pathology outline, to identify specific proteins expressed by different cell types. Positive markers commonly associated with mesothelioma include calretinin, WT1, D2-40, and CK5/6, while negative markers often include CEA, Ber-EP4, and MOC-31. However, no single marker is entirely specific, so a combination is always assessed. Adenocarcinomas, particularly those of lung origin, typically show the opposite staining pattern. The pathology outline clearly states which markers were used, their staining intensity and distribution, and the overall interpretation, allowing clinicians to confidently differentiate mesothelioma from other malignancies, which is essential for appropriate treatment selection.
What are the key prognostic factors that are typically included in mesothelioma pathology outlines, and how do they impact patient outcomes?
Mesothelioma pathology outlines include several prognostic factors that help predict patient outcomes. These include the histological subtype (epithelioid mesothelioma generally has a better prognosis than sarcomatoid or biphasic), the presence and extent of necrosis, mitotic count (a measure of cell division rate), and the presence of lymphovascular invasion (cancer cells spreading into blood vessels or lymphatic vessels). The stage of the disease, as determined by imaging and surgical findings, is also a critical factor and is often correlated with the pathology findings. The pathology outline will also comment on the completeness of resection if surgery was performed. Higher mitotic counts, sarcomatoid histology, extensive necrosis, and lymphovascular invasion are typically associated with a poorer prognosis, while epithelioid histology and complete surgical resection often indicate a better outcome. These factors, detailed in the pathology outline, guide treatment decisions and help clinicians provide patients with realistic expectations regarding their prognosis.